Ghana Priorities: Fecal Treatment and Reuse
Technical Report
The Problem
In Ghana, the prevalence of onsite sanitation is more than 85%. This means that when the receptacles containing the faecal sludge are full they have to be collected and treated before discharging into the environment. Unfortunately, there are very few treatment plants available in the country and faecal sludge is mostly dumped into water bodies, drains, trenches, farms, bushes and other unauthorized places.
The danger of these practices is the pathogen load in human faeces. Poor end-of-pipe treatment poses a serious health challenge in the country. In 2017, it was estimated that there were 41 million cases of diarrhea and 7,300 related deaths in Ghana. A microbial risk analysis notes that 88% of diarrheal disease in Accra can be traced to poor sanitation, with only the remaining 12% to unsafe water. Another report indicated 75% of child deaths from cholera and diarrhea were the result of poor sanitation. Research had shown that the economic burden of diarrhea is considerable and one older estimate indicated that poor sanitation cost Ghana over $290 million in 2012, which at the time accounted for 1.6% of GDP.
Intervention 1: Comprehensive Treatment Plants
Overview
This intervention looks to build 18 treatment plants in major municipal and urban centers across the country, which would provide treatment services to some 6.8m people. This FSTP involves three stages called the primary, secondary and tertiary treatment. Modern technologies are employed in this type of intervention. The primary treatment includes the physical process of screening, grit removal and some sedimentation. The secondary treatment involves a physical phase separation to remove settleable solids and a biological process to remove dissolved and suspended organic loadings. The tertiary treatment is the final cleaning process that improves the wastewater quality before it is reused, recycled or discharged into the environment. Additionally the intervention involves the construction of a 2km access road and increased enforcement capacity to ensure trucks haul sludge to the plants for each site.
Implementation Considerations
The intervention would likely require collaboration between the public and private sector. Public-private partnership arrangements can be created that for example, mean that government provides some of the upfront capital and/or guarantees of enforcement, while the private sector operates and maintains the plants with payments based on meeting certain service standards. These arrangements would need to be negotiated on a case-by-case basis.
The calculations presented below assume that the failure rate is 5% in the second year, increasing by 5% every year before stabilizing at 50% after 10 years.
Costs and Benefits
Costs
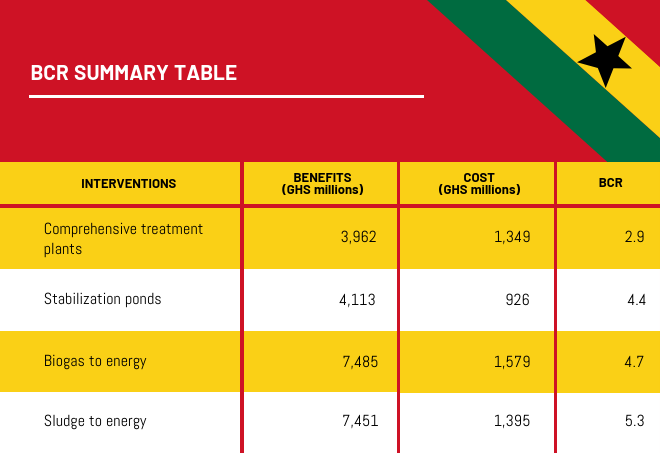
The intervention is estimated to cost 642m cedi in upfront investment and ongoing maintenance and operations cost of around 97m cedi in the first year. Over a period of 15 years, with assumed failure rate noted above, the present value of costs is 1,349m cedi with around 48% being upfront investments in capital, and the remainder in operations and maintenance.
Benefits
The intervention would avoid around 2m cases of diarrhea and 329 associated deaths in the first year, with benefits decreasing proportionally to the assumed failure rate of plants. The total benefits of the intervention are estimated at 3,962m cedi over 15 years.
Intervention 2a and 2b: Resource Recovery plants (gas-to-energy and sludge-to-energy)
Overview
This intervention assumes the building of plants across 64 locations across Ghana serving 14m people. It is a two-ended approach in management of faecal sludge. One part is the treatment aspect it provides in receiving the sludge and the second aspect is the recovery of energy provides. The resource recovery systems are in two folds; Biogas to electricity and Sludge to electricity. Additionally the intervention involves the construction of a 2km access road for each site and increased enforcement capacity to ensure trucks haul sludge to the plants.
Biogas to Electricity
This intervention involves the generation of biogas from faecal sludge and subsequent conversion of the biogas to electricity. The plant would have three key stages, the primary treatment stage, secondary treatment stage and then the electrical power generation stage. The primary treatment includes the physical process of screening and grit removal. The secondary treatment involves an anaerobic digestion process which would generate the biogas from the sludge, the biogas is purified and subsequently stored. The third component receives the purified biogas and the chemical energy of the combustible gases is converted to mechanical energy in a controlled combustion system by a heat engine. This mechanical energy then activates a generator to produce electrical power.
Sludge to Electricity
This intervention involves the use of mechanically screened faecal sludge to produce electricity through approved gasification and incineration technology. The plant would have a drying bed for the receipt of the faecal sludge, the combustion chamber unit and the appropriate extension of the power to the grid or internal use. The process involves drying the sludge and gasifying it, thus using the gas for electricity production. The leachate from the drying beds are subsequently treated, disinfected and discharged as effluent.
Implementation Considerations
The interventions would likely require collaboration between the public and private sector. Public-private partnership arrangements can be created that for example, mean that government provides some of the upfront capital and/or guarantees of enforcement, while the private sector operates and maintains the plants with payments based on meeting certain service standards. These arrangements would need to be negotiated on a case-by-case basis.
The calculations presented below assume that the failure rate is 5% in the second year, increasing by 5% every year before stabilizing at 50% after 10 years.
Costs and Benefits
Costs
A summarized version of the costs is presented in the table below for both options across 64 locations in Ghana. The costs are relatively similar for both biogas to electricity and sludge to electricity options with expected CAPEX equal to 784m cedi and 737m cedi respectively. Total opex is GHS 104m and GHS 97m respectively in the first year, and decreasing proportionally with the assumed failure rate.
Over a 15-year period, the estimated costs are GHS 1,579 million and GHS 1,395 million respectively for biogas to energy and sludge to energy.
Costs of resource recovery options across 64 locations in Ghana
| Population served | Total capex (GHS, millions) | Total opex in the first year (GHS, millions) | |
|---|---|---|---|
| Biogas to Electricity | 13,994,704 | 784 | 104 |
| Sludge to Electricity | 13,994,704 | 737 | 97 |
Benefits
The intervention would avoid around 3.8m cases of diarrhea and 591 associated deaths in the first year, with benefits decreasing proportionally to the assumed failure rate of plants. The estimated benefits are GHS 7,485 million and GHS 7,451 million respectively, for BCRs of 4.7 and 5.3. There are some electricity produce benefits embedded in these figures, but the share of total benefits is negligible.
Intervention 3: Stabilization Ponds
Overview
This intervention assumes the building of ponds across 46 locations in Ghana that would serve 6.8m people. It involves the use of traditional waste stabilization ponds in handling faecal sludge. This typically involves anaerobic, facultative and maturation. But with the intervention a primary treatment where physical screening process, grit removal and some sedimentation would be introduced before the anaerobic process starts. A multiple stage maturation pond system would be introduced for effective disinfection. Additionally the intervention involves the construction of a 2km access road for each site and increased enforcement capacity to ensure trucks haul sludge to the ponds.
Implementation Considerations
The intervention would likely require collaboration between the public and private sector. Public-private partnership arrangements can be created that for example, mean that government provides some of the upfront capital and/or guarantees of enforcement, while the private sector operates and maintains the plants with payments based on meeting certain service standards. These arrangements would need to be negotiated on a case-by-case basis.
The calculations presented below assume that the failure rate is 5% in the second year, increasing by 5% every year before stabilizing at 75% after 5 years.
Costs and Benefits
Costs
The intervention is estimated to cost 298m cedi in upfront investment and ongoing maintenance and operations cost of around 35m cedi in the first year. Over a period of 15 years, with assumed failure rate noted above, the present value of costs is 926m cedi with around a third being upfront investments in capital, and the remainder in operations and maintenance.
Benefits
The intervention would avoid around 1.9 million cases of diarrhea and 263 deaths in the first year, with benefits decreasing proportionally to the assumed failure rate of plants. The total benefits of the intervention are estimated at 4,113m cedi over 15 years.