Ghana Priorities: Nutrition
Technical Report
The Problem
Ghana is considered one of the few success stories on the African continent regarding child nutrition. The rates of child growth faltering (indicated as stunting, wasting, and underweight) has declined steadily at the national level (GSS et. al., 2014). Trend data from the Demographic and Health Survey (DHS) and multiple Indicator Cluster Survey (MICS) demonstrate that the rate of stunting (indicating chronic undernutrition) among children below five years has declined significantly from 35% in 2003 to 19% in 2017, at the national level (GSS et. al., 2014; MICS, 2018). The rate of wasting (indicating acute undernutrition) has declined, almost by half, from 8% to 5% in the same period. The number of underweight children (indicating low weight compared to normal weight children of similar age) also has declined from 18% in 2003 to 11% (GSS et. al., 2014; GMHS, 2018).
It is, however, important to note that the rates of undernutrition in young children in Ghana remains unacceptably high, especially when compared to other countries at a similar developmental stage. Further, although the national prevalence of these undernutrition indicators has declined, there are wide differences across rural and urban settings, regions, income levels, and education levels that are yet to be addressed. Another important aspect of child nutrition is the prenatal stage. The proportion of children born with a low birth weight (<2500g) has remained around 10% (GSS et. al., 2014).
Intervention 1: Multiple Micronutrients and Calcium in Pregnancy
Overview
Avoidable maternal deaths are unacceptably high in Ghana. An estimated 310 women die per 100,000 live births, annually (GSS et. al., 2017). Between 10% and 20% of maternal deaths in Ghana are due to hypertensive disorders, particularly pre-eclampsia and eclampsia (Asamoah et. al., 2011; Der EM et. al., 2013). There is an indication that the calcium status of pregnant women in Ghana may be lower than non-pregnant counterparts (Djagbletey et. al., 2018). Additionally, anemia among pregnant women is an important health and nutrition challenge in Ghana; an estimated 42% of women are anemic (IGSS et. al., 2014; Ghana Micronutrient Survey, 2017).
Implementation Considerations
The intervention analyzed calls for the provision of multiple micronutrient (MMN) and calcium (Ca) supplements at routine antenatal care (ANC) visits. Currently, MMN and Ca supplementation is not a routine public health policy in Ghana. However, based on WHO recommendation, Ghana has been implementing iron and folate (IFA) supplementation, and there is an experience in the Ghana Health Service for delivering IFA supplements through the health system with significant success. Currently, 89% of pregnant women undertake at least four ANC visits and 93% of pregnant women take IFA supplements during pregnancy (GSS et. al., 2014). Given that MMN and Ca represent a similar type of product as IFA delivered in a setting with high patronage by pregnant women (ANC visits), the basis for a successful intervention is strong. Based on this, we anticipate that the intervention coverage will range from 64% to 98% of pregnant women, with a base case estimate of 89%. After accounting for still-births, we estimate that a total of 850,573 pregnant women will be reached by the intervention (i.e. will be given the supplements) out of which 791,033 (93%) will actually take them.
Costs and Benefits
Costs
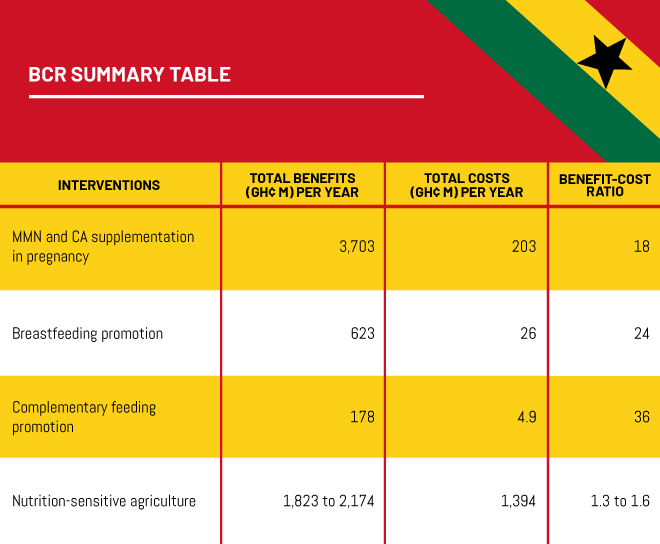
We estimate the monthly tablet cost for MMN and Ca respectively as 0.5 and 28.16 GH¢ in 2018 prices. Applying this cost to all 850,573 women estimated to have been reached by the intervention and assuming an 8-month course, the total ongoing costs for the intervention is estimated at GH¢ 203 million, representing over 96% of the total costs of this intervention.
Benefits
The analysis indicates a range of substantial benefits from the intervention including 109,637 cases of avoided anemia, 24,162 cases of avoided pre-term birth, and 82 avoided maternal deaths. Further, in total, the intervention is expected to avoid 3,951 infant deaths, 82 maternal deaths, and 887 stillbirths.
Intervention 2: Breastfeeding Promotion
Overview
Early initiation (within the first hour of birth) and exclusive breastfeeding during the first six months is recommended for infant survival and optimal development. However, rates of both early initiation and exclusive breastfeeding have stagnated. A recent assessment of the barriers to scaling-up breastfeeding in Ghana identified a number of challenges including insufficient funding and capacity to sustain breastfeeding promotion all year-round, and inadequate human resource capacity to deliver effective services (Aryeetey et. al., 2018).
Implementation Considerations
This intervention focuses on breastfeeding counseling delivered in facility- and community-based settings and improving the competence (knowledge and skills) of health care providers to counsel caregivers and their significant others on breastfeeding. This will be achieved through training and providing job aids such as counseling cards, guidance protocols, plus monitoring and evaluation. In addition, the intervention aims to increase the coverage of baby-friendly hospitals which were initiated in Ghana in 1993 to improve optimal breastfeeding (UNICEF, 2017). However, implementation of the initiative in Ghana is suboptimal (Aryeetey et. al., 2013).
Costs and Benefits
Costs
Direct costs of breastfeeding promotion include i) training of health workers, ii) community support, iii) training in breastfeeding code implementation and iv) baby friendly hospitals. The total cost for these four components is $26.75 (2015 Int$) per live birth, which corresponds to GH¢ 60 in 2018 prices. 56% of the unit cost is for baby friendly hospital implementation, 37% for community support and 7% for the remaining two components. This cost is applied to all 173,764 women who receive the intervention. The total direct cost of promotion is therefore GH¢ 10.4 million.
The time cost of breastfeeding promotion factors in six consultations of 30 minutes from each mother over the course of pre- and post-pregnancy, with most of the consultations occurring after birth. The value of women’s time is based on Ghana Priorities’ standard assumptions of half of relevant wage and is equal to GH¢ 3.25 / hour. This time cost is applied against all women who receive the intervention and totals GH¢ 1.4 million. Further a time cost of one hour per day is assumed for women who exclusively breastfeed because of the intervention and would have otherwise not breastfed or partially breastfed.
Benefits
The analysis indicates that 745 child deaths would be avoided from the intervention over two years, based on a target population of approximately 174,000 women with 43,300 women adhering to exclusive breastfeeding, and 20,600 continuing to breastfeed until 2 years. Further, the analysis indicates that the intervention will avoid 158,370 cases of diarrhea over two years with most of the cases avoided, coming from upper respiratory infections. The results indicate that benefits are equal to approximately GH¢ 622M with 98% of benefits coming from mortality avoided.
Intervention 3: Complementary Feeding Promotion
Overview
Optimal complementary feeding involves providing young children with sufficient quantities of quality diets at sufficient frequency, appropriate to age (Dewey et. al., 2008). This is achieved through providing diets which are sufficiently diverse (that is varied) food groups and at optimal frequency, based on child age. Dietary counseling for young infants assumes that caregivers are food secure and that the deficits in child feeding is dependent on improving caregiver competence on optimal foods and feeding methods. For those who are food insecure, complementary feeding promotion is not effective without combining dietary counseling with a food provisioning strategy (WHO, 2003), and will not be considered in this analysis.
Implementation Considerations
This intervention provides information about complementary feeding to caregivers through child welfare clinics in Ghana through one-on-one dietary counseling. Although the intervention targets all children attending child welfare clinics, those whose growth pattern trails behind the growth standard, are more likely to benefit from dietary counseling. Scaling up complementary feeding promotion requires multiple actions including training of care providers on how to use existing counseling cards, and on counseling skills. Complementary feeding intervention also requires increasing supply of job aids for dietary counseling. The intervention targets 173,764 children (in households which are food secure), representing a 20% increase in the coverage of the intervention.
Costs and Benefits
Costs
Based on Ghana Priorities’ assumptions, we calculate the cost of reaching a child as GH¢ 28 (at 2018 prices). We also include the cost of mother’s time and following Penny et al. (2005), Saleem et al. (2014) and Zhang et al. (2013), assume about 7 counseling sessions of one hour duration per mother. We also used personnel time per counseling session of 0.17 hour (or 10 minutes) following Bhutta et al. (2013). The cost of maternal time is also valued at Ghana Priorities standard assumptions and equals GH¢ 2.7 per hour. The total cost of the intervention is GH¢ 4.9m of which GH¢ 4.6m represents direct promotion costs and the remainder maternal time costs.
Benefits
The results of the analysis indicate that the intervention will avoid 65 deaths, with 27 deaths avoided in the period between 6-11 months, and the remaining deaths over the next four years. Diarrhea disease and lower respiratory infections represent the causes with the greatest deaths avoided. The central estimate of benefits from the intervention is GH¢ 178m with 73% of the benefits from increased productivity, and 27% from improved health benefits.
Intervention 4: Nutrition-Sensitive Agriculture
Overview
Globally, sub-optimal diets, and malnutrition in all its forms are common and linked with disease and impaired health outcomes. A critical aspect of improving the food and nutrition system is to better understand the important role agriculture plays in supplying adequate amounts of quality food in a sustainable fashion across different contexts. Agricultural strategies that address malnutrition (nutrition-sensitive agriculture) are considered critical to address malnutrition.
Implementation Considerations
The intervention is a community-based integrated health and nutrition-sensitive agriculture intervention targeting households. The agriculture component of the intervention involves providing inputs to eligible households (those with young children under one year old). The households receive thirty to forty chickens at point of lay that will be raised for their eggs. Along with the chickens, they also receive technical assistance for constructing chicken coop, maintaining health, hygiene, and reducing mortality of the chickens, harvesting, storing and marketing the eggs. Beneficiary households also receive support for identifying a sustainable source of feed as well as increasing/replacing their chicken stock, when needed. The intervention also included a substantial home gardening component to provide households with nutritious vegetable-based foods.
Costs and Benefits
Costs
The costs of the intervention are based on a recent analysis that estimated both financial and economic costs of the intervention delivered to 287 households. Total costs of the intervention are GH¢ 8,025 per household with 45% of the costs for education and training, 38% for poultry production, and the remainder for home gardens. Given a population of ~174,000 households, the total costs of the intervention would equal GH¢ 1,394m
Benefits
The results of the analysis estimate three types of benefits –health and productivity benefits from avoided stunting, as well as an increase in income from the intervention. It would generate GH¢ 1,823m in income benefits. The intervention reduces the prevalence of stunting in the beneficiary population by 5% leading to potential additional benefits for health (GH¢ 150m) and lifetime productivity (GH¢ 261m). We do not know how much of the extra income was used to generate the stunting reduction, and therefore we estimate a range of benefits between GH¢ 1,823m and GH¢ 2,174.