Ghana Priorities: Urban Sanitation
Technical Report
The Problem
Urban sanitation coverage in Ghana like in many other developing countries is low with only 25% of the people with access to basic sanitation (improved, non-shared sanitation) (Appiah-Effah et al., 2019). Already, poor urban sanitation is strongly linked to increased disease burdens and associated cost (Berendes et al., 2018; Prüss-Ustün et al., 2019).
Poor sanitation situation is attributed to several barriers including the main issues of lack of appropriate and affordable sanitation technologies especially for the urban poor (low-income groups), and poor enforcement of existing regulations like the local authorities bylaws (WSUP, 2017c; Antwi-Agyei et al., 2019). Other attributable reasons include high population densities and compelling demand for rental accommodation instead of toilets, poor physical planning, lack of rights over land as disincentive for sanitation infrastructure investments, mismatch between low-income levels and high cost of toilet facilities (Obeng et al., 2015).
The current urban sanitation situation is compelling and demands immediate attention from policy and decision makers to commit resources for remedial intereventions. The facts from the analysis of the most recent data – the Ghana Maternal Health Survey (MHS) 2017 speak explicitly:
- More than 10 million people, or 58% of urban households, live in housing in which more than 3 households share a toilet facility.
- Consequently, as many as 38% of urban households use public toilets, and
- 7.5% practice open defecation (OD).
- Such housing is rental units in compound houses with anywhere from 2-3 to well over 10 households.
The impacts of this poor sanitation situation include increased incidence of diarrheal morbidity and mortality, productive time loss (due to toilet access time, and illnesses), and large monetary cost in payment for public toilet usage. Several approaches to solving urban sanitation challenges have been experimented in Ghana. However, none is adopted at scale probably because little or not much is evidenced about their benefits and costs.
Intervention 1: Toilet subsidy provision with improved enforcement of sanitation by-laws
Overview
This intervention looks at providing toilet construction subsidy for urban households and/or compounds in addition to supporting Metropolitan, Municipal and District Assemblies (MMDAs) to enforce sanitation by-laws. While the subsidy attempts to lessen the cost burden of building improved household toilets, the enforcement component will incentivize households and/or landlords to meet up their contributions to the subsidies provided.
Implementation Considerations
The intervention will involve setting up program offices, carrying out promotion and awareness campaigns, giving out toilet subsidies, and supporting environmental health officers to effect sanitation regulation enforcement. The target population is urban households and/or compounds who are practicing open defecation, using uimproved facilities, using public toilet, and those who are sharing toilet with more than three households. This target reflects a two-staged approach in which a maximum of three households may share a toilet as an immediate interim improvement measure for compound sanitation challenges. The intervention improves sanitation situation by moving households to at worst three households sharing an improved toilet. Recent most popular urban toilet facility, the biodigestor toilet is the main technology for consideration. The subsidy provided is equivalent to the cost of this toilet facility of approximately GHS 4000. It is assumed in the analysis in this paper that implementation could have the following success or compliance rates: 100%, 75% and 50% uptake. Benefits and costs are assessed over a 20-year period are discounted at an annual rate of 5%, 8%, and 14% with a base case of 8%.
Costs and Benefits
Costs
The present value of the intervention cost, over a 20-year period, is between GHS 8.6 and 25.8 billion depending on compliance rate and discount rate. About 22 – 35% of intervention cost is borne directly by government (implementer of the intervention – cost of sanitation promotion program, enforcement and toilet), and the rest (65 – 78%) is paid by beneficiaries (landlords/households) in a form of toilet O&M, toilet cleaning, and foregone rental space. The most significant cost component at all times is foregone rental space accounting for 38 – 44% of the total intervention cost (GHS 3.2 – 11.4 billion).
Benefits
The present value of benefits from the intervention over the 20-year period is valued between GHS 34 and 107 billion. The largest share is productivity benefits from time savings amounting to GHS 23 – 68.4 billion (i.e. 63 – 70% of total benefits). Cost savings from no longer having to pay for public toilet usage is also high at GHS 6.8 to 24.1 billion, representing 19 – 24% of total benefits. Health benefits of averted mortality and morbidity contribute 11 – 13% of benefits from the intervention.
Intervention 2: Toilet subsidy provision only
Overview
This intervention only provides subsidy for toilets but without any emphasis on and budget for enforcement of sanitation bylaws. The subsidy equivalent to the 100% toilet cost is to lessen the burden of high cost of installing toilet facilities in urban compounds due to the loss of rental income from having to convert rental space into space for toilet facilities. In this intervention, no attention is given to enforcement moreover, the existing enforcement regime is expected to continue as business as usual without the intervention directly seeking any improvement.
Implementation Considerations
This intervention is similar to the first already presented. Thus, reproducing almost the same cost components except no cost for enforcement. The target population is same as the first intervention. In actual implementation like the first one, households and landlords will pay operation and maintenance (O&M) cost, toilet cleaning, and in most instance incurring the cost of foregone income from rental space released for toilet installation. It is expected that there will be comparatively low success or sanitation response rates associated with subsidy without enforcement because of the high cost besides the cost of toilets. Assessed intervention response rates are 20%, 10% and 1%. \
Costs and Benefits
Costs
The present value of total intervention cost is between GHS 0.23 and 5.1 billion depending on discount rate and sanitation response rate. About 21 – 52% of intervention cost is borne directly by government in the form of sanitation promotion program cost and toilet capital cost, and the rest (48 – 79%) is incurred by landlords/households as cost associated with toilet cleaning, operations and maintenance (O&M), and foregone rental space. Again, foregone rental space is accounting for a high proportion 28 – 44% (GHS 0.06 – 2.3 billion) of the total intervention cost.
Benefits
The present value of the benefits from the subsidy only intervention is between GHS 0.7 and 28.3 billion. The largest benefit, as for the previous intervention, is productivity benefits coming from time savings at GHS 0.6 – 20.6 billion, representing 72 – 74% of the overall benefits. This is followed by cost savings from no longer having to use public toilets (GHS 0.14 – 4.8 billion), representing 16 – 18% of total benefits. Health benefits of averted mortality and morbidity account for 9 – 10% of intervention benefits.
Benefit-cost ratios (BCRs)
The BCRs are slightly higher for the Subsidy provision only intervention (4.14 to 5.20 at the base case discount rate of 8%) than for the Subsidy with enforcement (3.87 – 4.55 at 8% discount rate) (BCR Summary Table). This is because the Subsidy only intervention has no enforcement cost. However, the net benefits of the subsidy with enforcement are substantially higher as sanitation compliance rates are likely to be substantially higher.
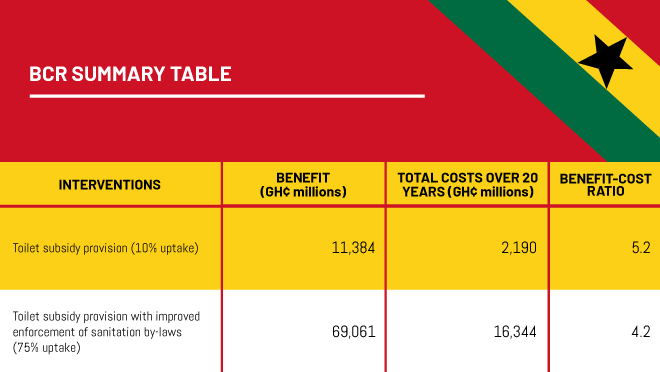
The quality of evidence supporting the evaluation process for the interventions is medium to strong looking at the nature and sources of data used in the assessment (BCR Summary Table).